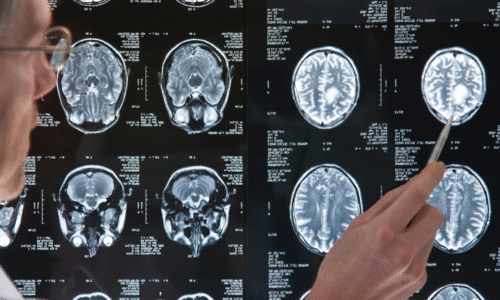
Doctors classify astrocytomas from Grade 1 to 4 based on how the tumor cells look and behave under a microscope, combined with modern molecular testing. The higher the grade, the more aggressive the tumor – meaning it grows faster and invades surrounding brain tissue more readily. Here’s a quick overview of the four grades:
- Grade I – Pilocytic Astrocytoma: This is the least aggressive type, often considered benign. It typically occurs in children or teens. Grade I tumors grow very slowly and stay fairly localized (they do not infiltrate broadly in the brain). If completely removed by surgery, a Grade I astrocytoma can often be cured and may not require chemo or radiation. (Grade I is relatively rare in adults.)
- Grade II – Diffuse Astrocytoma: This is a low-grade tumor found more often in adults (young adults, 20s-40s). “Diffuse” means it infiltrates into surrounding brain tissue (unlike Grade I, which is well-contained). Grade II astrocytomas grow slowly and the cells look only mildly abnormal. Often, patients might have subtle symptoms or seizures for years. Grade II can sometimes be monitored initially if it’s small and not causing problems, but it can progress to a higher grade over time (sometimes taking several years). Therefore, early surgery may be recommended.
- Grade III – Anaplastic Astrocytoma: “Anaplastic” means the cells are dividing rapidly. This is a high-grade malignant tumor. Grade III astrocytomas could arise from a prior lower-grade tumor that has become more aggressive, though they can also appear initially at Grade III. Under the microscope, these tumors have more densely packed cells and more cells actively dividing than Grade II. They lack the dead tissue areas seen in Grade IV, but they are still fast-growing and infiltrative. Grade III tumors almost always require treatment (surgery plus additional therapy) without delay. To be sure about Grade, a biopsy is needed.
- Grade IV – Glioblastoma: This is the most aggressive astrocytoma, a malignant brain cancer that tends to grow very rapidly and invasively. Glioblastomas can either evolve from lower-grade tumors or (more commonly) start as Grade IV outright (these are often IDH-wildtype GBMs in older adults). Under the microscope, GBM cells look very abnormal and chaotic, and the tumor contains areas of necrosis (dead cells) and new blood vessel growth – signs of how fast it’s growing, as it outgrows its blood supply. Glioblastoma is the most common primary malignant brain tumor in adults and unfortunately carries the poorest prognosis (we will discuss specifics on survival shortly).
Tumor grades I through IV visualized on a spectrum from least aggressive (Grade I, green) to most aggressive (Grade IV, red). Lower-grade astrocytomas (I-II) grow more slowly and are often well-contained, whereas higher-grade astrocytomas (III-IV) grow faster, spread more, and show more abnormal microscopic features. The arrow indicates increasing tumor aggressiveness →.
What Factors Determine the Grade?
When a pathologist examines the tumor tissue, they look for certain features that distinguish a low-grade from a high-grade tumor. Key factors include:
- Cellularity: How densely packed the tumor cells are. Low-grade tumors tend to have cells that are only slightly more numerous than normal brain, whereas high-grade tumors have crowded sheets of tumor cells. Higher cellularity usually means a more aggressive tumor.
- Cell Atypia: How abnormal the cells look under the microscope. Pathologists check if the cells have irregular shapes, large dark nuclei, etc. Grade increases with cellular abnormality (atypia).
- Mitotic activity: How many cells are actively dividing. This is seen by counting mitoses (cell divisions) on the slides. Grade II tumors have few dividing cells, while Grade III and IV have many (sign of faster growth). In fact, “anaplastic” Grade III by definition has high mitotic activity.
- Microvascular proliferation: Are there new blood vessels forming within the tumor? High-grade astrocytomas often stimulate the growth of new, abnormal blood vessels to feed the tumor. This angiogenesis is typically seen in Grade IV (and sometimes III). It’s one of the features pathologists used in older criteria to define glioblastoma.
- Necrosis: Is there dead tissue within the tumor? This is a hallmark of Grade IV (glioblastoma). The presence of necrosis means the tumor is growing so fast parts of it are dying – a clear sign of Grade IV malignancy. Lower-grade astrocytomas (grades II and III) do not have necrosis.
- Genetic markers : Today, doctors don’t just look at tumor cells under a microscope—they also examine genetic and molecular markers to better understand the tumor’s behavior and guide treatment. These markers are now a core part of how astrocytomas and glioblastomas are classified.
- IDH mutation (Isocitrate Dehydrogenase): One of the most important markers. Tumors with an IDH mutation (IDH-mutant)—often seen in Grade II or III astrocytomas—tend to grow more slowly and have a better prognosis. If a tumor lacks this mutation (IDH-wildtype) and has other aggressive features, it is often classified as glioblastoma (GBM).
- MGMT promoter methylation: This marker doesn’t affect tumor grade but is essential for predicting how well the tumor will respond to chemotherapy (especially temozolomide). When the MGMT gene is methylated, patients often respond better to treatment.
- TERT promoter mutation: Frequently seen in IDH-wildtype GBMs, this mutation helps the tumor maintain its ability to keep growing and is associated with a more aggressive disease.
- EGFR amplification or EGFRvIII mutation: A common alteration in GBM that promotes tumor growth. Researchers are exploring targeted therapies against this marker in clinical trials.
- CDKN2A deletion: Often found in high-grade tumors, this deletion removes a key tumor suppressor gene and is linked to faster progression and worse outcomes.
- 1p/19q co-deletion: Although more commonly associated with oligodendrogliomas, this combined chromosomal loss helps doctors distinguish between different types of gliomas and can guide both diagnosis and treatment planning.
- Together, these molecular markers provide a more accurate picture of the tumor and allow your care team to tailor treatment specifically to your case—a major advance in personalized medicine for brain tumors.
Don’t worry if this sounds technical. In essence, Grade II tumors look closer to normal brain and lack aggressive signs; Grade III tumors look more abnormal and proliferative; Grade IV tumors look the most aggressive with dead areas and chaotic growth. These features also guide treatment – for example, a Grade IV glioblastoma requires very aggressive therapy, whereas a small Grade II tumor might be watched for a while if it’s not causing symptoms.
Sources: This guide is based on current medical literature and patient education resources (updated 2025), including expert input from MD Anderson Cancer Center, the American Association of Neurological Surgeons, and recent research findings in oncology. All medical information has been reviewed for accuracy and is intended for educational purposes. Always consult your physician for advice tailored to your situation. Stay hopeful and informed – science is making strides against astrocytomas and glioblastomas every day.
Find Advanced Treatment on our Website under Study Finder
Download the Wetrials App to learn more.